Office of Research & Development |
 |
Talk to the Veterans Crisis Line now
An official website of the United States government


Army Veteran Robert Lewis, wearing a myoelectric arm, peruses a magazine at the VA Pittsburgh Healthcare System. (Photo by Bill George)
February 20, 2020
Mike Richman
VA Research Communications
A new study finds similar levels of satisfaction among Veteran users of upper-limb prostheses regardless of which type of device they use.
The results appeared online in the journal Prosthetics and Orthotics International in January 2020.
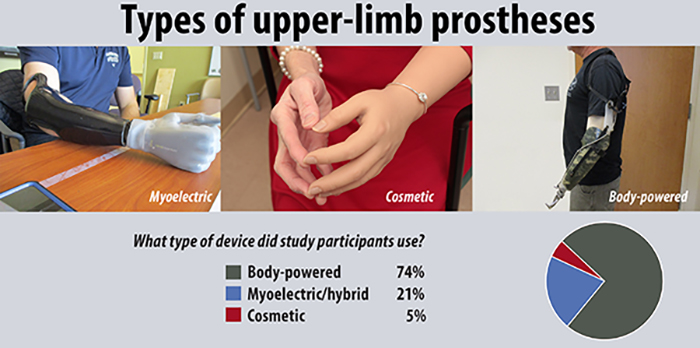
In a survey of more than 400 Veterans, the researchers found little difference in satisfaction, at the group level, among users of myoelectric, body-powered, and cosmetic prostheses. Overall across the three groups, the average rankings fell just shy of “satisfied.”
A myoelectric prosthesis is an externally powered artificial limb that is controlled with electrical signals generated by one’s muscles. The device can replace missing hands, elbows, and shoulders, depending on the level of amputation. The most advanced experimental systems can transmit sensation back to the user in the case of fingers and touch, a feature that is not available in commercial devices.
"Many people have expectations about what these devices should do that just aren't being met."
A body-powered device is operated by a cable. Movement of another part of the body, such as the shoulder blades, pulls the cable open and controls the limb.
Cosmetic prostheses are used by upper- and lower-limb amputees for appearance purposes. Older designs are often a kind of vinyl, while more recent ones are made from urethanes and silicones that closely reflect the appearance of the natural limb.
The researchers also observed no satisfaction difference based on the type of terminal device, which is the prosthetic hook or hand. The most commonly used prostheses have hooks or hands that open and close in one position. Advanced prosthetic hands with multiple degrees of freedom allow the user to move the hand into different grasping positions.

VA engineering research center posts another invention: prosthetic hook mouse

VA scientists testing new technology to absorb moisture, increase comfort with prostheses

Researchers piloting nerve stimulation for amputation pain
Dr. Linda Resnik of the Providence VA Medical Center led the study. She and her colleagues expected to see greater satisfaction with people using myoelectric devices that provide multiple degrees of freedom. She was thus surprised to find no difference in prosthesis satisfaction.
“I thought that people who got the newest and the latest and greatest devices that offer multiple degrees of freedom would be happier with them,” says Resnik, who is also affiliated with Brown University in Rhode Island. “There could be many reasons we didn’t find that. These devices are known to be more fragile. The more mechanically complicated devices are, the more places they can break. So they may end up being in the shop more. Many people have expectations about what these devices should do that just aren’t being met.”
Resnik and her team also aimed to identify factors linked to prosthesis satisfaction. They found that initial prosthetic training was associated with greater happiness, pointing to the “critical role of occupational or physical therapy in the early stages of prosthetic care.”
“That training usually includes hours and hours of practice using it, learning strategies to use it, and learning how to incorporate the prosthesis into your everyday activities,” Resnik explains. “That’s what physical therapists and occupational therapists do. It’s hard to believe, but data show that some people don’t receive training to use their devices. When that happens, patients don’t incorporate their device into their daily lives, as well. They become frustrated and are set up for a bad experience. Early training is very important for later satisfaction.
“Some medical centers don’t have the expertise to provide the right training,” she adds. “That’s a problem with a lot of specialized rehabilitation and training protocols. Clinicians don’t see enough patients to develop the right expertise. VA has some advantages. We have a national amputation system of care with regional amputation centers. Also, VA can offer tele-rehab and consultation.”
In additional findings, the researchers observed that the proximal level, which is the closeness of the amputated limb to the frame of the body, was linked to lower satisfaction levels. The shoulder is closer than the elbow or wrist, for example. This finding was consistent with past literature that showed people with amputation at the shoulder level had the highest rate of device rejection (60%), followed by those who had the procedure above the elbow (57%), and those with an amputation below the elbow (6%).
“The more joints you lose, basically the harder it is to replace the function of the arm,” Resnik says. “If you lose your shoulder, for example, it’s really difficult to replace that kind of movement. Your shoulder is critical to getting the hand placed in different positions. The weight of the prosthesis gets progressively heavier, too, depending on how long it is and how many components it includes. So it’s pretty well known that people with more proximal amputations tend to abandon devices because they don’t feel like they restore enough function and because they think they’re not worth the effort.”
Resnik has been working in upper-limb prosthetic development for more than a decade. The field can be very complex, with no one-size-fits-all solution that satisfies everyone. She has studied some of the most sophisticated technologies, including the LUKE/DEKA arm, which was the first prosthetic arm with the ability to perform simultaneous powered movements. VA researchers were key to testing and optimizing the LUKE/DEKA arm, which the U.S. Food and Drug Administration approved in 2014. In comparing that device to existing prostheses, she became interested in the capabilities of other technologies. She has been trying to understand which devices people are happiest with and which ones are most functional.
Her latest study is part of a larger national survey published last year. The survey covers many aspects of Veteran prosthesis use and care received. “That’s what motivated me to do this study,” she says. “It was working on the development of new technologies and realizing that we don’t know what today’s upper-limb prostheses can do or how people feel about what’s available.”
This year’s study included 429 Veterans with an upper-limb amputation who received VA care between 2010 and 2015. Seventy-four percent of the Veterans used body-powered devices, 21% myoelectric or hybrid, and 5% cosmetic. The sample was almost entirely male, and the average age was 63. Myoelectric users were the youngest group, with an average age of 56. A greater proportion of African-American participants were in the cosmetic group (36%). They made up 10% of both the myoelectric and body-powered groups.
The Veterans rated device satisfaction using two scales. One scale asked about the color, shape, noise, appearance, usefulness, reliability, fit, comfort, and overall satisfaction of the prosthesis. The ratings differed based on prosthesis type. For example:
The other scale included statements that the participants agreed or disagreed with. For instance:
The researchers modeled the outcomes from each of the scales separately. After adjusting for other factors that might influence satisfaction, such as amputation level and age, they found no differences in satisfaction.
One of the study’s limitations was that only eight of the participants were women, hindering the researchers’ ability to compare them to male prosthesis users. There are not many female Veterans with upper-limb amputation, and a smaller proportion use upper-limb prostheses as compared to males. Resnik has a paper comparing male and female Veteran upper-limb amputees that is now under review. She’s also leading a VA-funded study to assess prostheses satisfaction and acceptance levels among women with upper-limb amputation.
In other findings, Resnik and her team concluded that younger Veterans and those who are black were less satisfied with their prostheses. The connection between younger age and dissatisfaction, Resnik says, likely stems from that demographic having higher expectations and greater desires to be more active.
“Older people were more satisfied with their devices perhaps because, on average, they had been prosthesis users for the longest period of time and perhaps had come to value their devices,” Resnik says. “In general, as people age, they become more satisfied with life, and they have better mental health. That’s a known phenomenon. They may have different expectations of what they should be able to do. Perhaps younger people, they’re seeing the news, they’re hearing about the latest and greatest research, and some of the news stories make it seem like the newest prostheses should do everything that your arm and hand does.”
Resnik was not sure why African-American respondents were less satisfied. She and her colleagues plan to look deeper into that finding to understand the root cause.
While it’s known that many users of upper-limb prostheses are dissatisfied with their devices, that same sentiment—in Resnik’s opinion—isn’t necessarily shared by users of lower-limb prostheses.
“Upper limbs have so many functions,” she says. “We use our hands to interact with the world, to help ourselves with basic activities, washing and dressing and eating, and to communicate with other people. Think of all the places your hand goes in space to do different activities. It’s very complicated. The lower limbs, although they have a lot of functions, their primary function is to help you walk, run, sit, and stand. Those kinds of activities are easier to replicate. If you don’t yet have a prosthesis on your lower limb, you might be able to walk with an assisted device like a walker or crutches.
“Huge advances have been made to restore sensation with upper-limb prostheses,” she adds. “In the future, we will have functional and durable technologies that can restore the sense of touch. I expect that having such sensation will dramatically improve device satisfaction.”
Lewis uses a kiosk in the lobby of the VA Pittsburgh Healthcare System. (Photo by Bill George)
While in the Army in the early 1990s, Robert Lewis was in a car accident that led to the amputation of his left arm below the elbow.
These days, he uses two types of prostheses daily. His battery-powered myoelectric arm allows him to move his fingers and makes it easier to perform light activities, such as getting dressed or holding an object like a newspaper. He wears the device six to eight hours a day. For more stressful activities like hunting, fishing, or riding on rough terrain in an all-purpose vehicle, he’ll use his body-powered prosthesis, which is more durable and has a hook on the end. He may use that device up to 10 hours a day during the hunting season.
The way Lewis sees it, both technologies serve their purpose, but one isn’t better than the other. On a scale of 1 to 10, with 10 being the highest, he gives each one a rating of five.
“Nothing’s going to ever truly give you back your arm or your hand,” he says. “But without these devices, life would be a lot more difficult. As time goes on, these technologies are making things a little easier for me. I thank the good Lord that VA does for me what it can.”
His satisfaction level aligns with the conclusion in a VA study that found no difference in prosthesis satisfaction with the three most popular upper-limb technologies: myoelectric, body-powered, and cosmetic (see main story). Lewis, who also uses the myoelectric arm for cosmetic reasons because it looks more life-like, was one of the more than 400 Veterans who took part in the study. Dr. Linda Resnik of the Providence VA led the research.
To Lewis, both the myoelectric and body-powered devices present challenges.
“They both get a good bit of wear,” he says. “With the body-powered one, the strap hooks to the opposite shoulder. It’s strictly running off a cable. After wearing it for a couple of hours, you’ll feel discomfort around that shoulder and under your armpit. Your limb in the socket will start sweating sometimes. With the myoelectric one, I make sure I have an undershirt on. It also gets very sweaty, and the limb in the socket can get a little irritated. It will also put a little pressure on the elbow area after a couple of hours of use.”
Plus, he finds that the myoelectric battery runs out faster depending on how much he’s using his prosthetic hand, he says. More hand activity means the battery will last up to six hours, compared with eight hours with less intense movement. “It would be ideal if they could come out with a longer-lasting battery, maybe a lithium battery, that lasts up to 14 hours,” he says.
The body-powered prosthesis requires little maintenance, he adds, noting that the arm and hook are easy to wipe off. He makes sure the myoelectric hand doesn’t make contact with a liquid or with dirt, both of which could derail the device’s electrical components. “Something a little more durable with the myoelectric would be awesome,” he says.
Lewis is interested in testing a myoelectric device that the manufacturer, Taska Prosthetics, touts as the world’s first waterproof prosthetic hand. The technology is designed, for instance, to allow users to wash their hands without causing damage. Lewis says he hopes the hand would be more durable, compared with his current myoelectric prosthesis.
Despite his concerns, Lewis likes the robotic look of the myoelectric hand. Some amputees, he notes, use a flesh-colored rubber glove that’s made to look like one’s real skin. But he doesn’t mind if people notice he has a prosthetic hand. The prosthetic hand connects with a socket that slides into the arm, with sensors inside the socket sending a message to the wrist and the fingers. He has no sense of touch. But “the more you use it, the easier it will be to know how hard to squeeze something,” he says.
He stresses that It’s important to get a comfortable socket.
“I’ve had situations where I didn’t wear my devices because of discomfort,” he says, “and I wasn't aware of the difference one prosthetic clinic that makes a socket could make compared with another. But over time, I've realized that you should bring any discomfort to the attention of a [prosthetist] so the problem can be fixed. Comfort goes hand in hand with technology. If someone doesn't like the feel, then that person won’t use the device.”
Lewis thinks studies on upper-limb prostheses, such as the one led by Resnik, are long overdue.
“Those studies should have been done 20, 30 years ago, if not longer,” he says. “As far as advances in technology, there could have been something out there way better for upper-limb amputees. Lower-limb amputees have great products available to them, a lot more than what we have. Dr. Resnik’s study is going to help upper-limb amputees a lot in the future. If something benefits an amputee two to three years down the road, I’m all for it.”
--- Mike Richman
VA Research Currents archives || Sign up for VA Research updates